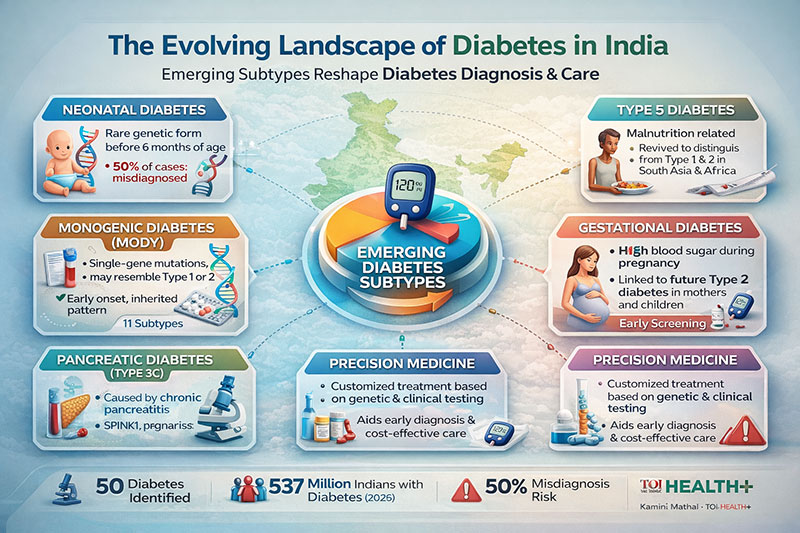
The diabetes crisis in India is not just a simple case of “juvenile” vs “adult-onset” disease anymore. According to Kamini Mathai in The Times of India, new study in genetics and medicine has found around 50 different varieties of diabetes, each with its own unique causes and treatment options. This growing classification is a big step toward precision therapy, which could change the way things work in a country that has the second highest number of adults with diabetes in the world.
For many years, diabetes was mostly divided into two types: Type 1 (autoimmune death of pancreatic beta cells) and Type 2 (mostly insulin resistance). In India, Type 2 still makes up around 90% of instances, whereas Type 1 makes up only 2%. But the report says that this kind of simplification could lead to wrong diagnoses and bad treatments, which can have serious effects.
A compelling example is neonatal diabetes, an uncommon monogenic disorder observed in infants under six months of age. Dr. V. Mohan, an endocrinologist, says that if the problem is accurately diagnosed, insulin medication can often be substituted with a cheap sulfonylurea. In the situation recounted, a youngster who was wrongly diagnosed with Type 1 diabetes needed five insulin injections a day, which cost too much. After genetic testing verified neonatal diabetes, treatment changed to one tablet a day, which made things more easier and less expensive for everyone.
This example strengthens the worldwide demand for personalized care. Dr. Mohan writes that “To a patient, a precise diagnosis of diabetes can feel like a miracle.” The World Health Organization has also said that controlling non-communicable diseases must move toward early detection and personalized treatment.
The article also talks about Type 5 diabetes, a new type of diabetes that the International Diabetes Federation (IDF) has acknowledged as being linked to malnutrition. This subtype is very important in some parts of South Asia and sub-Saharan Africa, and it is commonly mistaken for Type 1 or Type 2. But its metabolic profile is different; the amount of insulin it needs and the amount of beta-cell reserve it has are both different. Misclassification might result in excessive treatment or improper insulin utilization. Dr. Nihal Thomas says that “Getting the type right matters” because the wrong treatment can have catastrophic consequences.
From an Indian perspective, this has significant ramifications for public health. Childhood malnutrition persists in several places, potentially exposing millions to under-recognized forms of diabetes. Screening techniques must, therefore, be attuned to socioeconomic and dietary settings, not alone glycaemic readings.
Gestational diabetes mellitus (GDM) is another notable aspect. The paper says that around one in four women who go to government clinics in India have been diagnosed with GDM. New research reveals that many cases may happen earlier in pregnancy than they are presently checked for. Finding problems early could stop problems for mothers and babies. Organizations like the IDF and the American Diabetes Association have also stressed the importance of stricter glycaemic management during pregnancy to lower the long-term metabolic risk for children.
The fact that there are different forms of diabetes in different parts of the world makes things much more complicated. Page 7 of the report shows a side-by-side view: Scandinavian countries indicate a higher prevalence of Type 1 diabetes, Western countries show more alcohol-related pancreatic diabetes, and Black African individuals are more likely to develop ketosis. Type 3C diabetes, which is linked to chronic pancreatitis and genetic abnormalities like SPINK1, has been common in southern India, especially in Kerala. Patients may have gastrointestinal pain, diarrhoea, weight loss, and sugar levels that change a lot, which means they need both endocrine and exocrine pancreatic.
This difference between regions shows that diabetes is not a single thing, but a range of things. Sir William Osler famously observed, “Medicine is a science of uncertainty and an art of probability.” In the age of genetic medicine, that uncertainty is slowly going away.
Precision diabetology is part of a bigger trend toward individualized medicine around the world. Genetic screening for MODY (Maturity-Onset Diabetes of the Young) and pharmacogenomic customization of therapy are becoming more common in specialized practice in the US and Europe. As the article points out, making genetic testing more affordable in India can make these discoveries available to more people.
Three advisory priorities come to light from a policy point of view:
1. Improve diagnostic pathways: Primary care doctors should learn to look for unusual signs of diabetes, such as early onset, a strong family history, severe insulin sensitivity or resistance, or signs of malnutrition.
2. Make genetic testing more available: Public-private partnerships may help make testing for neonatal and monogenic diabetes inexpensive, which will stop people from having to use insulin for the rest of their lives.
3. Change the rules for screening: National programs need to include early screening for GDM and diabetes associated to malnutrition.
People have long called India’s diabetes problem a “tsunami.” But there is a chance in this catastrophe. The country can lead a new way of caring for diabetes by using subtype identification, combining genetics, and customizing treatment.
Swami Vivekananda wisely said, “Strength is life; weakness is death.” Getting the diagnosis right is not just a scientific breakthrough; it is also a moral duty. The Times of India article makes a strong case for the idea that we can get closer to fair, effective, and compassionate care for everyone with diabetes if we stop using simple labels and see how different the disease really is.
Dr. Prahlada N.B
MBBS (JJMMC), MS (PGIMER, Chandigarh).
MBA in Healthcare & Hospital Management (BITS, Pilani),
Postgraduate Certificate in Technology Leadership and Innovation (MIT, USA)
Executive Programme in Strategic Management (IIM, Lucknow)
Senior Management Programme in Healthcare Management (IIM, Kozhikode)
Advanced Certificate in AI for Digital Health and Imaging Program (IISc, Bengaluru).
Senior Professor and former Head,
Department of ENT-Head & Neck Surgery, Skull Base Surgery, Cochlear Implant Surgery.
Basaveshwara Medical College & Hospital, Chitradurga, Karnataka, India.
My Vision: I don’t want to be a genius. I want to be a person with a bundle of experience.
My Mission: Help others achieve their life’s objectives in my presence or absence!
Leave a reply















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave a reply