The worldwide lack of subspecialist knowledge is no longer just a guess; it is a fact of life. The World Health Organization says that by 2030, there will be 18 million fewer health workers than there are now. This will be especially hard on rural areas and those with few resources. This gap is especially harmful in cardiology, where a late diagnosis can lead to abrupt cardiac death. A new randomized controlled study published in Nature Medicine—“A large language model for complex cardiology care” by O’Sullivan et al.—provides a thorough assessment of the potential of large language models (LLMs) to address this gap.
A Randomized Test of AI-Assisted Cardiology
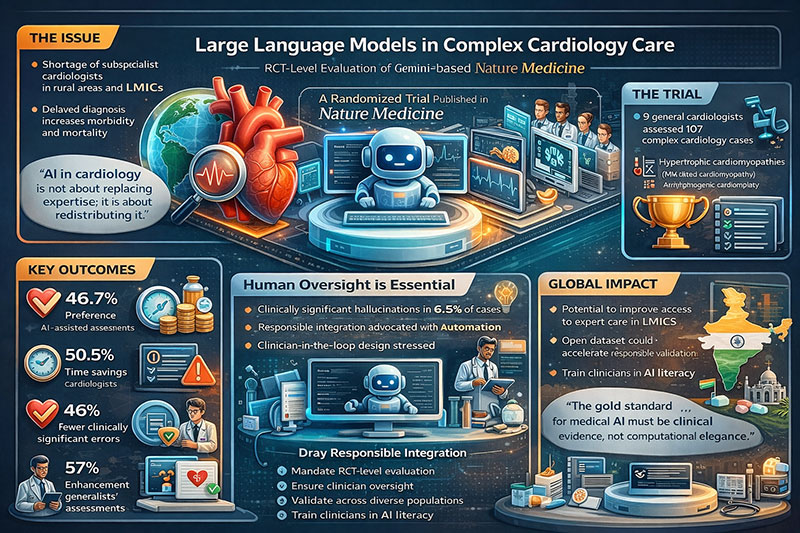
The study assessed the Articulate Medical Intelligence Explorer (AMIE), an LLM-based system developed on Gemini 2.0 Flash. Nine general cardiologists evaluated 107 actual cases of probable hereditary cardiomyopathies, encompassing hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy, and arrhythmogenic cardiomyopathy. Two cardiologists looked at each case separately, one with AMIE help and one without. Using a structured ten-domain rubric, blinded subspecialists looked at the outputs.
The findings were statistically and clinically significant. Subspecialists favored AMIE-assisted assessments in 46.7% of instances, in contrast to 32.7% for unassisted cardiologists (P = 0.02). The number of clinically significant errors went down from 24.3% to 13.1% (P = 0.033), and the number of missing content went down from 37.4% to 17.8% (P = 0.0021). Cardiologists said that AMIE helped them make better decisions in 57% of cases and saved them time in 50.5% of cases.
These results constitute one of the initial RCT-level assessments of LLM aid within a subspecialty domain, addressing a deficiency consistently emphasized in systematic reviews of medical AI.
Why Cardiology Is the Right Test Case
Inherited cardiomyopathies show how serious the stakes are. HCM is a major cause of sudden cardiac mortality in young adults. The report also says that more than half of U.S. states don’t have HCM subspecialty clinics and that more than 60% of people still don’t know they have the disease. The authors contend that LLMs may aid generalists in recognizing high-risk situations, enhancing triage, and improving management strategies.
This is very important from an Indian point of view. India is dealing with two problems: the number of people with heart disease is going up, and cardiology expertise is not evenly spread out, with much of it being in big cities. In Tier-2 and Tier-3 cities, general doctors and cardiologists who aren’t specialists are typically the only ones who can help. AI-assisted decision assistance could help make handling complicated cases more consistent and cut down on unneeded referrals and travel time.
One way to put it is, “AI in cardiology isn’t about replacing expertise; it’s about moving it around.” In low- and middle-income nations, where diagnostic imaging is becoming more common but specialized interpretation is still hard to get, these techniques could make the current infrastructure even better.
Human Supervision Is Still Necessary
The study does not endorse autonomous AI. Hallucinations that are important for medical purposes. These included made-up imaging results and wrong assumptions about the people involved. But when cardiologists questioned these results, AMIE often fixed itself. The authors warn against deploying too soon without supervision and point out the danger of automated bias.
This balanced framing is really important. The report points out that LLMs are already being added to electronic health record systems, even though there isn’t any similar RCT proof. The current trial serves as a methodological framework, characterized by thorough evaluation, blinded assessment, and open-source data access.
One thing is evident from throughout the world: “The gold standard for medical AI must be clinical evidence, not computational elegance.” By registering the trial (NCT06935253) and adhering to CONSORT criteria, the authors advance the conversation beyond mere hype to the realm of health systems science.
Equity, Data, and the Global South
But limits dampen enthusiasm. The dataset came from just one center in the U.S. and only had English-language text and a small range of demographic groups. The authors recognize that inequities in the management of hereditary cardiomyopathy are well established and that the evaluation of bias necessitates more comprehensive validation.
The challenge for India and other LMICs is not whether LLMs are effective in Silicon Valley cardiology clinics, but if they are applicable across diverse linguistic, socioeconomic, and epidemiological contexts. Local datasets, multilingual training, and compliance with regulations from organizations like the CDSCO and ICMR will be crucial.
Also, the open-source release of de-identified cardiac test data under CC 4.0 licensing gives people a chance to work together. Indian universities and AI research organizations might use this dataset to compare their own models to others, which would help science around the world.
From Help to Improvement
One interesting conclusion is that the biggest benefits were in management planning, not in diagnostic triage. This is in line with other recent RCTs mentioned in the discussion, which imply that LLMs may be better at putting together complex management paths than at coming up with initial differentials.
This difference is important for health systems. AI might be most useful as a cognitive scaffold, making sure that management plans are complete, that interventions based on guidelines are highlighted, and that mistakes are kept to a minimum. In a country like India, where there are a lot of patients and a lot of strain on time, even small decreases in omission errors could lead to big health advantages.
Advocacy: Responsible Integration
This experiment shows that something is possible, not that it is finished. It reveals that LLMs can help generalists learn new skills, make fewer mistakes, and work more quickly while they are being watched. It has not yet shown better results for patients.
So, advocacy ought to be based on principles:
1. Require RCT-level evaluation before widespread use.
2. Make sure that the physician is involved in the design to lower the likelihood of hallucinations.
3. Put money into local validation across a range of groups.
4. Include lessons on AI in cardiology training programs.
The authors conclude that AMIE “can improve general cardiologists’ assessments of complex cardiac patients”—but its complementary role necessitates additional investigation.
The message is both positive and cautious for India and the rest of the world: AI won’t fix the lack of workers on its own, but using evidence-based methods to improve clinical intelligence could make life-saving knowledge more available to everyone. The future of cardiology may not be a competition between machines and doctors, but rather a collaboration between the two, informed by science and governed by ethics.
Dr. Prahlada N.B
MBBS (JJMMC), MS (PGIMER, Chandigarh).
MBA in Healthcare & Hospital Management (BITS, Pilani),
Postgraduate Certificate in Technology Leadership and Innovation (MIT, USA)
Executive Programme in Strategic Management (IIM, Lucknow)
Senior Management Programme in Healthcare Management (IIM, Kozhikode)
Advanced Certificate in AI for Digital Health and Imaging Program (IISc, Bengaluru).
Senior Professor and former Head,
Department of ENT-Head & Neck Surgery, Skull Base Surgery, Cochlear Implant Surgery.
Basaveshwara Medical College & Hospital, Chitradurga, Karnataka, India.
My Vision: I don’t want to be a genius. I want to be a person with a bundle of experience.
My Mission: Help others achieve their life’s objectives in my presence or absence!
Leave a reply















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave a reply